FAQ
We are here to help you through every hurdle you face. We have anticipated a few queries you may have.
Know everything here because we have sorted everything out for you.
Ask us anything !

Infertility
Click Below to Know More
Ectopic Pregnancy
Click Below to Know More
Endometriosis
Click Below to Know More

Fibroids
Click Below to Know More
PCOS
Click Below to Know More
Cervical Cancer
Click Below to Know More

Pap Test
Click Below to Know More
Frequently Asked Questions About Infertility
What is infertility?
Infertility means not being able to get pregnant after one year of trying. Or,
six months, if a woman is 35 or older. Women who can get pregnant but are
unable to stay pregnant may also be infertile.
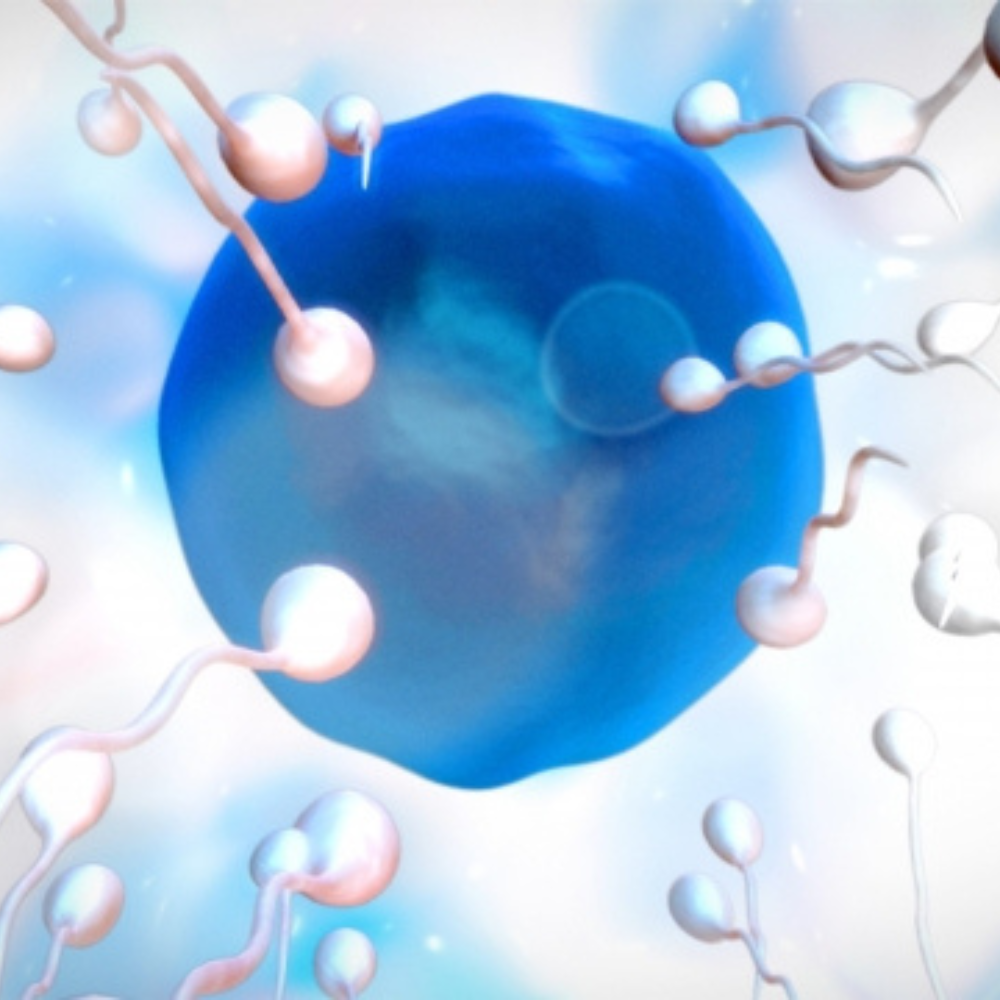
Pregnancy is the result of a process that has many steps. To get pregnant:
• A woman’s body must release an egg from one of her ovaries (ovulation).
• The egg must go through a fallopian tube toward the uterus (womb).
• A man's sperm must join with (fertilize) the egg along the way.
• The fertilized egg must attach to the inside of the uterus (implantation).
Pregnancy is the result of a process that has many steps. To get pregnant:
• A woman’s body must release an egg from one of her ovaries (ovulation).
• The egg must go through a fallopian tube toward the uterus (womb).
• A man's sperm must join with (fertilize) the egg along the way.
• The fertilized egg must attach to the inside of the uterus (implantation).
How common is it?
It affects 10-15% of couples. Or simply put, 1 in 7 couples are suffering from Infertility
Is it True that Infertility is caused mostly due to problems with of the female partner?
No. In general, Infertility can be attributed to the female partner one third of the time, the male partner one third of the time and both partners in the remaining one third.
What are the various causes of Infertility?
Female:
Conditions affecting the functioning of Ovaries, Fallopian tubes, Uterus or Hypothalamus.
Ovaries: Polycystic Ovarian Disease (PCOD), Premature Ovarian Failure, Diminished Ovarian Reserve, Chocolate cysts etc
Fallopian Tube: Blocked or distorted fallopian tubes as seen in Endometriosis and Infections
Uterus: Presence of Fibroids, Adenomyosis, Septum, Polyps etc
Hypothalamus: Extremes of weight, excessive physical or emotional stress
Male:
Disruption of Testicular & Ejaculatory function, as in Trauma/torsion of testes, varicocoeles, mumps in childhood and cancer treatment
Hormonal disorders
Genetic Disorders
Intake of steroid hormones like anabolic steroids and supplements
What are the reasons for increase in incidence of infertility today?
Some of the factors that have contributed are
Delaying age of childbearing
Increase in prevalence of sexually transmitted infections
Sedentary lifestyle & rising obesity
Smoking &alcohol
Increased levels of stress
Endocrine disrupting chemicals in environment
Is there any relationships of age with Infertility?
Yes. For women, optimal fertility is in their early &mid twenties. There is a gradual fall after age of thirty years and a sharp decline after the age of 35 years.
The quantity and quality of eggs is affected with increasing age of women. Further there is a higher risk of miscarriage and birth defects in the baby as age increases.
Couples in which the male partner is 40 years or older are more likely to report difficulty in conceiving.
When should couples seek consultations for it?
In general, infertility investigations are conducted after 1 year of trying to conceive. However for women aged 35 years or older, couples should see a doctor after 6 months of trying unsuccessfully.
Also couples with the following should consult earlier
Irregular periods
Painful periods
Known case of endometriosis
History of pelvic surgery
History of Tuberculosis
History of Cancer treatment
Which expert can manage Infertility more scientifically?
A qualified Obstetrician and Gynaecologist can treat Infertility. Also the expertise of an Urologist is sought to investigate and treat issues related to Male Infertility. However, patients needing Assisted Reproductive Techniques like Intra-Uterine Insemination (IUI) and In-Vitro Fertilization (IVF)may be referred to a fertility Specialists trained in these techniques.
Is infertility just a woman's problem?
No, infertility is not always a woman's problem. Both women and men can have problems that cause infertility. About one-third of infertility cases are caused by women’s problems. Another one third of fertility problems are due to the man. The other cases are caused by a mixture of male and female problems or by unknown problems
What increases a man's risk of infertility?
A man's sperm can be changed by his overall health and lifestyle. Some things that may reduce the health or number of sperm include:
• Heavy alcohol use
• Drugs
• Smoking cigarettes
• Age
• Environmental toxins, including pesticides and lead
• Heavy alcohol use
• Drugs
• Smoking cigarettes
• Age
• Environmental toxins, including pesticides and lead
What things increase a woman's risk of infertility?
Many things can change a woman's ability to have a baby. These include:
• Age
• Smoking
• Excess alcohol use
• Stress
• Poor diet
• Athletic training
• Being overweight or underweight
• Sexually transmitted infections (STIs)
• Age
• Smoking
• Excess alcohol use
• Stress
• Poor diet
• Athletic training
• Being overweight or underweight
• Sexually transmitted infections (STIs)
How will doctors find out if a woman and her partner have fertility problems?
Doctors will do an infertility checkup. This involves a physical exam. The doctor will also ask for both partners’ health and sexual histories. Sometimes this can find the problem. However, most of the time, the doctor will need to do more tests.
In men, doctors usually begin by testing the semen. They look at the number, shape, and movement of the sperm. Sometimes doctors also suggest testing the level of a man's hormones.
What is assisted reproductive technology (ART)?
Assisted reproductive technology (ART) is a group of different meth ods used to help infertile couples. ART works by removing eggs from a woman's body. The eggs are then mixed with sperm to make embryos. The embryos are then put back in the woman's body.
How often is assisted reproductive technology (ART) successful?
Success rates vary and depend on many factors. Some things that affect the suc cess rate of ART include:
• Age of the partners
• Reason for infertility
• Clinic
• Age of the partners
• Reason for infertility
• Clinic
What are the different types of assisted reproductive technology (ART)?
Common methods of ART include:
• In vitro fertilization (IVF) means fertilization outside of the body. IVF is the most effective ART. It is often used when a woman's fallopian tubes are blocked or when a man produces too few sperm. Doctors treat the woman with a drug that causes the ovaries to produce multiple eggs. Once mature, the eggs are removed from the woman. They are put in a dish in the lab along with the man's sperm for fertilization. After 3 to 5 days, healthy embryos are implanted in the woman's uterus
• Intracytoplasmic sperm injection (ICSI) is often used for couples in which there are serious problems with the sperm. Sometimes it is also used for older couples or for those with failed IVF attempts. In ICSI, a single sperm is injected into a mature egg. Then the embryo is transferred to the uterus or fallopian tube.
ART procedures sometimes involve the use of donor eggs (eggs from another woman), donor sperm, or previously frozen embryos. Donor eggs are sometimes used for women who can not produce eggs. Also, donor eggs or donor sperm is sometimes used when the woman or man has a genetic disease that can be passed on to the baby. An infertile woman or couple may also use donor embryos. These are embryos that were either created by couples in infertility treatment or were created from donor sperm and donor eggs. The donated embryo is transferred to the uterus. The child will not be genetically related to either parent.
Surrogacy Women with no eggs or unhealthy eggs might also want to consider surrogacy. A surrogate is a woman who agrees to become pregnant using the man's sperm and her own egg. The child will be genetically related to the surrogate and the male partner. After birth, the surrogate will give up the baby for adoption by the parents. Gestational Carrier Women with ovaries but no uterus may be able to use a gestational carrier. This may also be an option for women who shouldn't become pregnant because of a serious health problem. In this case, a woman uses her own egg. It is fertilized by the man's sperm and the embryo is placed inside the carrier's uterus. The carrier will not be related to the baby and gives him or her to the parents at birth.
• In vitro fertilization (IVF) means fertilization outside of the body. IVF is the most effective ART. It is often used when a woman's fallopian tubes are blocked or when a man produces too few sperm. Doctors treat the woman with a drug that causes the ovaries to produce multiple eggs. Once mature, the eggs are removed from the woman. They are put in a dish in the lab along with the man's sperm for fertilization. After 3 to 5 days, healthy embryos are implanted in the woman's uterus
• Intracytoplasmic sperm injection (ICSI) is often used for couples in which there are serious problems with the sperm. Sometimes it is also used for older couples or for those with failed IVF attempts. In ICSI, a single sperm is injected into a mature egg. Then the embryo is transferred to the uterus or fallopian tube.
ART procedures sometimes involve the use of donor eggs (eggs from another woman), donor sperm, or previously frozen embryos. Donor eggs are sometimes used for women who can not produce eggs. Also, donor eggs or donor sperm is sometimes used when the woman or man has a genetic disease that can be passed on to the baby. An infertile woman or couple may also use donor embryos. These are embryos that were either created by couples in infertility treatment or were created from donor sperm and donor eggs. The donated embryo is transferred to the uterus. The child will not be genetically related to either parent.
Surrogacy Women with no eggs or unhealthy eggs might also want to consider surrogacy. A surrogate is a woman who agrees to become pregnant using the man's sperm and her own egg. The child will be genetically related to the surrogate and the male partner. After birth, the surrogate will give up the baby for adoption by the parents. Gestational Carrier Women with ovaries but no uterus may be able to use a gestational carrier. This may also be an option for women who shouldn't become pregnant because of a serious health problem. In this case, a woman uses her own egg. It is fertilized by the man's sperm and the embryo is placed inside the carrier's uterus. The carrier will not be related to the baby and gives him or her to the parents at birth.
Are there any necessary tests before deciding to go with IUI?
Prior to initiating IUI treatment, women must have at least one documented open fallopian tube as demonstrated by hysterosalpingogram, or the tubal dye study.
What is IUI?
Intra uterine insemination (IUI) is a procedure wherein specially prepared sperms are inserted into the woman’s uterus. IUI is often used to treat mild male-factor infertility and unexplained infertility.
What is IVF?
In vitro Fertilization procedure involves removing mature eggs from a woman’s ovaries using a needle, combining the eggs with sperm in the laboratory and returning the embryos so formed back to the woman’s uterus.
Is it true that couples must undergo many repetitive and expensive tests?
No. Basic investigations like semen analysis and hormonal profilesare generally advised during initial consultation and are not repeated unless abnormal. However, some patients may need more detailed investigations like Hysterosalpingography (HSG), Hysteroscopy and Laparoscopy.
Are there any steps that can be taken to avoid Infertility?
The following can help avoid Infertility
Maintaining a healthy lifestyle with regular exercise and good eating habits
Avoiding Smoking, Alcohol and recreational drugs
Promoting prevention , early detection and treatment of sexually transmitted diseases
Reducing exposure to environmental toxins and chemicals like dioxins, pesticides, lead, disphenol-A, phthalates (commonly found in plastics)
Frequently Asked Questions About Pap Test
What is a Pap test?
The Pap test, also called a Pap smear, checks for changes in the cells of your cervix. The cervix is the lower part of the uterus (womb) that opens into the vagina (birth canal). The Pap test can tell if you have an infection, abnormal (unhealthy) cervical cells, or cervical cancer.
Why do I need a Pap test?
A Pap test can save your life. It can find the earliest signs of cervical cancer. If caught early, the chance of curing cer vical cancer is very high. Pap tests also can find infections and abnormal cervi cal cells that can turn into cancer cells. Treatment can prevent most cases of cervical cancer from developing. Getting regular Pap tests is the best thing you can do to prevent cervical cancer. In fact, regular Pap tests have led to a major decline in the number of cervical cancer cases and deaths.
Do all women need Pap tests?
It is important for all women to have Pap tests, along with pelvic exams, as part of their routine health care. You need a Pap test if you are 21 years or older.Women who have gone through meno-pause (when a woman’s periods stop) still need regular Pap tests. Women ages 65 and older can talk to their doctor about stopping after at least 3 normal Pap tests and no abnormal results in the last 10 years.
How often do I need to get a Pap test?
It depends on your age and health his-tory. Talk with your doctor about what is best for you. Most women can follow these guidelines:
• Starting at age 21, have a Pap test every 2 years.
• If you are 30 years old and older and have had 3 normal Pap tests for 3 years in a row, talk to your doctor about spacing out Pap tests to every 3 years.
• If you are over 65 years old, ask your doctor if you can stop having Pap tests.
Ask your doctor about more frequent testing if:
• You have a weakened immune system because of organ transplant, chemotherapy, or steroid use
• Your mother was exposed to diethylstilbestrol (DES) while pregnant
• You are HIV-positive Women who are living with HIV, the virus that causes AIDS, are at a higher risk of cervical cancer and other cervical diseases. The U.S. Centers for Disease Control and Prevention recommends that all HIV-positive women get an initial Pap test, and get re-tested 6 months later. If both Pap tests are normal, then these women can get yearly Pap tests in the future.
• Starting at age 21, have a Pap test every 2 years.
• If you are 30 years old and older and have had 3 normal Pap tests for 3 years in a row, talk to your doctor about spacing out Pap tests to every 3 years.
• If you are over 65 years old, ask your doctor if you can stop having Pap tests.
Ask your doctor about more frequent testing if:
• You have a weakened immune system because of organ transplant, chemotherapy, or steroid use
• Your mother was exposed to diethylstilbestrol (DES) while pregnant
• You are HIV-positive Women who are living with HIV, the virus that causes AIDS, are at a higher risk of cervical cancer and other cervical diseases. The U.S. Centers for Disease Control and Prevention recommends that all HIV-positive women get an initial Pap test, and get re-tested 6 months later. If both Pap tests are normal, then these women can get yearly Pap tests in the future.
Who does not need regular Pap tests?
The only women who do not need regular Pap tests are:
• Women over age 65 who have had 3 normal Pap tests and in a row and no abnormal test results in the last 10 years, and have been told by their doctors that they don’t need to be tested anymore.
• Women who do not have a cervix and are at low risk for cervical cancer. These women should speak to their doctor before stopping regular Pap tests.
• Women over age 65 who have had 3 normal Pap tests and in a row and no abnormal test results in the last 10 years, and have been told by their doctors that they don’t need to be tested anymore.
• Women who do not have a cervix and are at low risk for cervical cancer. These women should speak to their doctor before stopping regular Pap tests.
I had a hysterectomy. Do I still need Pap tests?
It depends on the type of hysterectomy (surgery to remove the uterus) you had and your health history. Women who have had a hysterectomy should talk with their doctor about whether they need routine Pap tests.
Usually during a hysterectomy, the cervix is removed with the uterus. This is called a total hysterectomy. Women who have had a total hysterectomy for reasons other than cancer may not need regular Pap tests. Women who have had a total hysterectomy because of abnormal cells or cancer should be tested yearly for vaginal cancer until they have three normal test results. Women who have had only their uterus removed but still have a cervix need regular Pap tests. Even women who have had hysterectomies should see their doctors yearly for pelvic exams.
How do I prepare for a Pap test?
Many things can cause wrong test results by washing away or hiding abnormal cells of the cervix. So, doctors suggest that for 2 days before the test you avoid:
● Douching
● Using tampons
● Using vaginal creams, suppositories, and medicines
● Using vaginal deodorant sprays or powders
● Having sex
● Douching
● Using tampons
● Using vaginal creams, suppositories, and medicines
● Using vaginal deodorant sprays or powders
● Having sex
Should I get a Pap test when I have my period?
No. Doctors suggest you schedule a Pap test when you do not have your period. The best time to be tested is 10 to 20 days after the first day of your last period.
How is a Pap test done?
Your doctor can do a Pap test during a pelvic exam. It is a simple and quick test. While you lie on an exam table, the doctor puts an instrument called a speculum into your vagina, opening it to see the cervix. She will then use a special stick or brush to take a few cells from inside and around the cervix. The cells are placed on a glass slide and sent to a lab for examination. While usually painless, a Pap test is uncomfortable for some women.
When will I get the results of my Pap test?
Usually it takes 3 weeks to get Pap test results. Most of the time, test results are normal. If the test shows that some-thing might be wrong, your doctor will contact you to schedule more tests. There are many reasons for abnormal Pap test results. It usually does not mean you have cancer.
What do abnormal Pap test results mean?
It is scary to hear that your Pap test results are “abnormal.” But abnormal Pap test results usually do not mean you have cancer. Most often there is a small problem with the cervix. Some abnormal cells will turn into cancer. But most of the time, these unhealthy cells will go away on their own. By treating these unhealthy cells, almost all cases of cervical cancer can be prevented. If you have abnormal results, to talk with your doctor about what they mean.
My Pap test was “abnormal,” what happens now?
There are many reasons for “abnormal” Pap test results. If results of the Pap test are unclear or show a small change in the cells of the cervix, your doctor will probably repeat the Pap test.
If the test finds more serious changes in the cells of the cervix, the doctor will suggest more powerful tests. Results of these tests will help your doctor decide on the best treatment. These include:
● Colposcopy: The doctor uses a tool called a colposcope to see the cells of the vagina and cervix in detail.
● Endocervical curettage: The doctor takes a sample of cells from the endocervical canal with a small spoon-shaped tool called a curette.
● Biopsy: The doctor removes a small sample of cervical tissue. The sample is sent to a lab to be studied under a microscope.
The FDA recently approved the LUMA Cervical Imaging System. The doctor uses this device right after a col poscopy. This system can help doctors see areas on the cervix that are likely to contain precancerous cells. The doctor uses this device right after a colposcopy. This system shines a light on the cervix and looks at how different areas of the cervix respond to this light. It gives a score to tiny areas of the cervix. It then makes a color map that helps the doctor decide where to further test the tissue with a biopsy. The colors and patterns on the map help the doctor tell between healthy tissue and tissue that might be diseased.
● Colposcopy: The doctor uses a tool called a colposcope to see the cells of the vagina and cervix in detail.
● Endocervical curettage: The doctor takes a sample of cells from the endocervical canal with a small spoon-shaped tool called a curette.
● Biopsy: The doctor removes a small sample of cervical tissue. The sample is sent to a lab to be studied under a microscope.
The FDA recently approved the LUMA Cervical Imaging System. The doctor uses this device right after a col poscopy. This system can help doctors see areas on the cervix that are likely to contain precancerous cells. The doctor uses this device right after a colposcopy. This system shines a light on the cervix and looks at how different areas of the cervix respond to this light. It gives a score to tiny areas of the cervix. It then makes a color map that helps the doctor decide where to further test the tissue with a biopsy. The colors and patterns on the map help the doctor tell between healthy tissue and tissue that might be diseased.
My Pap test result was a “false positive.” What does this mean?
Pap tests are not always 100 percent correct. False positive and false negative results can happen. This can be upsetting and confusing. A false positive Pap test is when a woman is told she has abnormal cervical cells, but the cells are really normal. If your doctor says your Pap results were a false positive, there is no problem.
A false negative Pap test is when a woman is told her cells are normal, but in fact, there is a problem with the cervical cells that was missed. False negatives delay the discovery and treatment of unhealthy cells of the cervix. But, having regular Pap tests boosts your chances of finding any problems. If abnormal cells are missed at one time, they will probably be found on your next Pap test.
For more information talk to your reproductive medicine specialist today. Dr Sachin Narvekar MD (O&G),FRM,is an endoscopy and fertility consultant attached to Vrundavan Hospital. He has undergone postdoctoral fellowship training in Reproductive Medicine from Bangalore. He was working as a consultant at Bangalore Assisted Conception and has performed a number of endoscopy and IVF (test tube baby) procedures. After returning to Goa he has established the assisted conception unit at Vrundavan Hospital Santa-Cruz.Dr Narvekar has published a number of research papers in this field. He is the member of Indian Society for Assisted reproduction
For more information talk to your reproductive medicine specialist today. Dr Sachin Narvekar MD (O&G),FRM,is an endoscopy and fertility consultant attached to Vrundavan Hospital. He has undergone postdoctoral fellowship training in Reproductive Medicine from Bangalore. He was working as a consultant at Bangalore Assisted Conception and has performed a number of endoscopy and IVF (test tube baby) procedures. After returning to Goa he has established the assisted conception unit at Vrundavan Hospital Santa-Cruz.Dr Narvekar has published a number of research papers in this field. He is the member of Indian Society for Assisted reproduction
Frequently Asked Questions About Fibroids
What are fibroids?
Fibroids are muscular tumors that grow in the wall of the uterus (womb). Another medical term for fibroids is “leiomyoma” (leye-oh-meye-OH-muh) or just “myoma”. Fibroids are almost always benign (not cancerous). Fibroids can grow as a single tumor, or there can be many of them in the uterus. They can be as small as an apple seed or as big as a grapefruit. In unusual cases they can become very large.
Why should women know about fibroids?
About 20 percent to 80 percent of women develop fibroids by the time
they reach age 50. Fibroids are most common in women in their 40s and early 50s. Not all women with fibroids have symptoms. Women who do have symptoms often find fibroids hard to live with. Some have pain and heavy menstrual bleeding. Fibroids also can put pressure on the bladder, causing frequent urination, or the rectum, causing rectal pressure. Should the fibroids get very large, they can cause the abdomen (stomach area) to enlarge, making a woman look pregnant.
Who gets fibroids?
There are factors that can increase a woman's risk of developing fibroids.
● Age. Fibroids become more common as women age, especially during the 30s and 40s through menopause. After menopause, fibroids usually shrink.
● Family history. Having a family member with fibroids increases your risk. If a woman’s mother had fibroids, her risk of having them is about three times higher than average.
● Ethnic origin. African-American women are more likely to develop fibroids than white women.
● Obesity. Women who are overweight are at higher risk for fibroids. For very heavy women, the risk is two to three times greater than average.
● Eating habits. Eating a lot of red meat (e.g., beef) and ham is linked with a higher risk of fibroids. Eating plenty of green vegetables seems to protect women from developing fibroids.
● Age. Fibroids become more common as women age, especially during the 30s and 40s through menopause. After menopause, fibroids usually shrink.
● Family history. Having a family member with fibroids increases your risk. If a woman’s mother had fibroids, her risk of having them is about three times higher than average.
● Ethnic origin. African-American women are more likely to develop fibroids than white women.
● Obesity. Women who are overweight are at higher risk for fibroids. For very heavy women, the risk is two to three times greater than average.
● Eating habits. Eating a lot of red meat (e.g., beef) and ham is linked with a higher risk of fibroids. Eating plenty of green vegetables seems to protect women from developing fibroids.
Where can fibroids grow?
Most fibroids grow in the wall of the uterus. Doctors put them into three groups based on where they grow:
● Submucosal (sub-myoo-KOH-zuhl) fibroids grow into the uterine cavity.
● Intramural (ihn-truh-MYOOR-uhl) fibroids grow within the wall of the uterus.
● Subserosal (sub-suh-ROH-zuhl) fibroids grow on the outside of the uterus.
Some fibroids grow on stalks that grow out from the surface of the uterus or into the cavity of the uterus. They might look like mushrooms. These are called pedunculated (pih-DUHN-kyoo-lay-ted) fibroids.
● Submucosal (sub-myoo-KOH-zuhl) fibroids grow into the uterine cavity.
● Intramural (ihn-truh-MYOOR-uhl) fibroids grow within the wall of the uterus.
● Subserosal (sub-suh-ROH-zuhl) fibroids grow on the outside of the uterus.
Some fibroids grow on stalks that grow out from the surface of the uterus or into the cavity of the uterus. They might look like mushrooms. These are called pedunculated (pih-DUHN-kyoo-lay-ted) fibroids.
What are the symptoms of fibroids?
Most fibroids do not cause any symptoms, but some women with fibroids can have:
● heavy bleeding (which can be heavy enough to cause anemia) or painful periods
● feeling of fullness in the pelvic area (lower stomach area)
● enlargement of the lower abdomen
● frequent urination
● pain during sex
● lower back pain
● complications during pregnancy and labor, including a six-time greater risk of cesarean section
● reproductive problems, such as infertility, which is very rare
● heavy bleeding (which can be heavy enough to cause anemia) or painful periods
● feeling of fullness in the pelvic area (lower stomach area)
● enlargement of the lower abdomen
● frequent urination
● pain during sex
● lower back pain
● complications during pregnancy and labor, including a six-time greater risk of cesarean section
● reproductive problems, such as infertility, which is very rare
What causes fibroids?
No one knows for sure what causes fibroids. Researchers think that more than one factor could play a role. These factors could be:
● hormonal (affected by estrogen and progesterone levels)
● genetic (runs in families) Because no one knows for sure what causes fibroids, we also don't know what causes them to grow or shrink. We do know that they are under hormonal control—both estrogen and progesterone. They grow rapidly during pregnancy, when hormone levels are high. They shrink when anti-hormone medication is used. They also stop growing or shrink once a woman reaches menopause.
● hormonal (affected by estrogen and progesterone levels)
● genetic (runs in families) Because no one knows for sure what causes fibroids, we also don't know what causes them to grow or shrink. We do know that they are under hormonal control—both estrogen and progesterone. They grow rapidly during pregnancy, when hormone levels are high. They shrink when anti-hormone medication is used. They also stop growing or shrink once a woman reaches menopause.
Can fibroids turn into cancer?
Fibroids are almost always benign (not cancerous). Rarely (less than one in 1,000) a cancerous fibroid will occur. This is called leiomyosarcoma (leye-oh-meye-oh-sar-KOH-muh). Doctors think that these cancers do not arise from an already-existing fibroid. Having fibroids does not increase the risk of developing a cancerous fibroid. Having fibroids also does not increase a woman’s chances of getting other forms of cancer in the uterus
Are all fibroids the same?
Fibroids can differ with respect to their size, location, number and by the symptoms that they can produce.
Uterine fibroids are generally classified as:
Subserous - growth is directed outwards
Intramural - growth centred within the uterine walls
Submucosal - growth towards the cavity of uterus
Rarely, fibroids can also form in cervix and broad ligament of uterus. The size of the fibroids does not seem to be related to the severity of the symptoms. So even a small fibroid (especially submucosal type) can cause considerable symptoms and sometimes a woman with a large fibroid may be asymptomatic.
Subserous - growth is directed outwards
Intramural - growth centred within the uterine walls
Submucosal - growth towards the cavity of uterus
Rarely, fibroids can also form in cervix and broad ligament of uterus. The size of the fibroids does not seem to be related to the severity of the symptoms. So even a small fibroid (especially submucosal type) can cause considerable symptoms and sometimes a woman with a large fibroid may be asymptomatic.
Who is most likely to develop fibroids?
Approximately 60 to 80% of women will have fibroids. The following are some of the risks factors for uterine fibroids:
Obesity (obese women produce more estrogen)
Early age at first periods
Family history of fibroids in mother or sister
Metabolic syndrome( diabetes+hypertension+high cholesterol+obesity)
Women with polycystic ovarian disease and irregular periods Age (older women are at higher risk than younger women )
Obesity (obese women produce more estrogen)
Early age at first periods
Family history of fibroids in mother or sister
Metabolic syndrome( diabetes+hypertension+high cholesterol+obesity)
Women with polycystic ovarian disease and irregular periods Age (older women are at higher risk than younger women )
How are fibroids formed?
The exact cause of fibroids is not well understood but multiple factors play a role in their growth.
Genetics
Estrogen and progesterone hormones
Environment and lifestyle
Genetics
Estrogen and progesterone hormones
Environment and lifestyle
What are symptoms in women having fibroids?
Most women with fibroids are asymptomatic.
However, some may have the following symptoms:
1.Changes in menses
Heavy menstrual bleeding
Painful menses ( cramps)
Irregular bleeding
These women are generally anemic (low hemoglobin) and complain of easy fatigue.
2.Pressure of fibroids on surrounding organs can cause
Difficulty in passing urine or frequent urination
Difficult bowel movements
Abdominal cramps
Back pressure on kidneys causing swelling of kidneys(hydronephrosis)
Feeling full in the belly
3.Pain
Dull ,aching pain in abdomen and lower back
Pain during sexual intercourse
4.Difficulty getting pregnant
5.Problems during pregnancy like miscarriage, preterm birth and pain in abdomen
Feeling lump in abdomen or increase in girth of abdomen
However, some may have the following symptoms:
1.Changes in menses
Heavy menstrual bleeding
Painful menses ( cramps)
Irregular bleeding
These women are generally anemic (low hemoglobin) and complain of easy fatigue.
2.Pressure of fibroids on surrounding organs can cause
Difficulty in passing urine or frequent urination
Difficult bowel movements
Abdominal cramps
Back pressure on kidneys causing swelling of kidneys(hydronephrosis)
Feeling full in the belly
3.Pain
Dull ,aching pain in abdomen and lower back
Pain during sexual intercourse
4.Difficulty getting pregnant
5.Problems during pregnancy like miscarriage, preterm birth and pain in abdomen
Feeling lump in abdomen or increase in girth of abdomen
What tests are done to diagnose uterine fibroids?
Unless a woman has symptoms, it is unlikely that she knows she has fibroids. They can sometimes be detected during routine pelvic examination done by a gynecologist.
Some common types of investigations done are
Ultrasound- mainstay of diagnosis.
MRI indicated in large and multiple fibroids
Hysteroscopy uses a small camera to visualize the inside of uterus
Ultrasound- mainstay of diagnosis.
MRI indicated in large and multiple fibroids
Hysteroscopy uses a small camera to visualize the inside of uterus
Is it true that pregnant woman with fibroids have complications in pregnancy?
Yes. The following problems may be encountered during pregnancy and childbirth
Pain: especially in large fibroids more than 5 cm
Recurrent miscarriage
Preterm birth
Premature separation of placenta (abruption)
More chances of baby being in abnormal position (breech,oblique) thus requiring caesarean delivery.
Excessive bleeding after delivery of baby .
Generally in pregnancy, fibroids can grow in 30% of patients, shrink in 30% and remain unchanged in 30%. The above mentioned complications are usually seen in patients with multiple fibroids and in whom the fibroids have grown during pregnancy. In the remaining, pregnancy may be uneventful.
Pain: especially in large fibroids more than 5 cm
Recurrent miscarriage
Preterm birth
Premature separation of placenta (abruption)
More chances of baby being in abnormal position (breech,oblique) thus requiring caesarean delivery.
Excessive bleeding after delivery of baby .
Generally in pregnancy, fibroids can grow in 30% of patients, shrink in 30% and remain unchanged in 30%. The above mentioned complications are usually seen in patients with multiple fibroids and in whom the fibroids have grown during pregnancy. In the remaining, pregnancy may be uneventful.
If I have fibroids, will it be difficult to get pregnant ?
Fibroids can impact fertility in the following cases
Submucosal fibroids which grow and bulge in uterine cavity
Multiple fibroids distorting the normal cavity and architecture of uterus
Fibroids near the tubal opening or in cervical canal.
However it is prudent to also evaluate other causes of infertility before attributing the issue to fibroids.
Submucosal fibroids which grow and bulge in uterine cavity
Multiple fibroids distorting the normal cavity and architecture of uterus
Fibroids near the tubal opening or in cervical canal.
However it is prudent to also evaluate other causes of infertility before attributing the issue to fibroids.
When is treatment necessary for fibroid uterus?
Several factors are considered before recommending treatment to a patient viz;
Age
Severity of symptoms
Location, size and number of fibroids
General health of the patient
Whether patient is desiring pregnancy in future
Fibroids that are small and do not cause any symptoms may not need treatment. However surveillance will be important by regular check-up or ultrasound, to watch for increase in size or any obstructive symptoms. This is especially important in a woman nearing menopause where the hormone levels drop and the fibroid may shrink on its own.
Certain conditions which necessitate treatment are:
1.Heavy , painful, irregular menstrual bleeding
2.Uncertainty whether the growth is a fibroid or another type of tumor, such as an ovarian tumor.
3.Rapid increase in growth of fibroid
4.Infertility
Obstructive urinary and intestinal symptoms
Age
Severity of symptoms
Location, size and number of fibroids
General health of the patient
Whether patient is desiring pregnancy in future
Fibroids that are small and do not cause any symptoms may not need treatment. However surveillance will be important by regular check-up or ultrasound, to watch for increase in size or any obstructive symptoms. This is especially important in a woman nearing menopause where the hormone levels drop and the fibroid may shrink on its own.
Certain conditions which necessitate treatment are:
1.Heavy , painful, irregular menstrual bleeding
2.Uncertainty whether the growth is a fibroid or another type of tumor, such as an ovarian tumor.
3.Rapid increase in growth of fibroid
4.Infertility
Obstructive urinary and intestinal symptoms
Can medicines be used to treat fibroids?
Medications can be used as a temporary option in some women to reduce pain and bleeding. Some newer medicines may also help to shrink fibroids. However they have to be taken only under strict medical supervision.
What type of surgery is done for fibroids?
Myomectomy is the surgical removal of fibroids leaving the uterus in place.
It can be done endoscopically (laparoscopy or hysteroscopy) or open surgery.
Hysterectomy is the removal of uterus. Laparoscopic and open surgery options are available.
Do fibroids turn Cancerous?
Fibroids are almost always benign (non cancerous)
Very rarely (less than 1 in 2000) a cancerous fibroid called leiomyosarcoma can occur.
Can fibroids be prevented?
Though they can’t be totally prevented, certain lifestyle habits can reduce your chances of developing fibroids. Regular exercise can help. So also, include plenty of fruits and vegetables in diet. Avoid alcohol, red meat, processed foods and refined sugars. Remember, excess body fat is an important risk factor for fibroids.
I believe our Lifestyle is a major determinant of Health and well being.
Frequently Asked Questions About An Ectopic Pregnancy
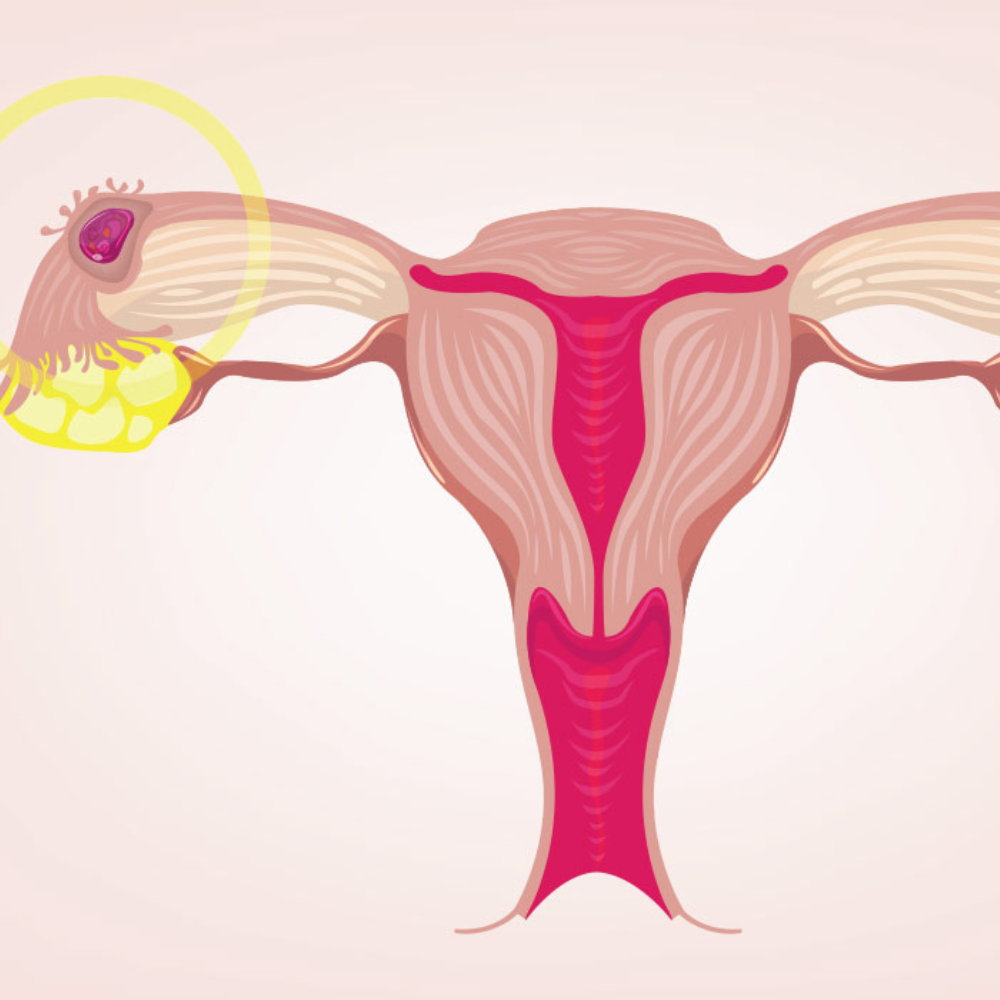
What is an ectopic pregnancy?
An ectopic pregnancy (literally means “out
of place”) is any pregnancy that grows outside
of its normal implantation site in the uterus.
In a normal conception, the egg is fertilized by
the sperm inside the fallopian tube and the
resulting embryo travels through the tube and
reaches the uterus 4 to 5 days later. The embryo
attaches itself to the endometrium of the uterus
and grows.
In an ectopic pregnancy the developing embryo
does not implant on the endometrial wall, but
instead attaches to some other surface
(commonly the fallopian tube). If not diagnosed
early, it can eventually lead to rupture causing
severe internal bleeding, shock and rarely death
of the woman.
Which are common sites for an ectopic pregnancy?
Fallopian tube ectopic pregnancies account
for more than 90% of all ectopics.
Pregnancy in previous cesarean section scar
(scar ectopic) and cervix is also common.
Rare sites are in the uterine cornua, ovaries and
abdomen.
What are the causes of ectopic pregnancy?
1. Tubal disease is the most common cause.
Infections like tuberculosis cause structural and
functional damage of the fallopian tubes,
predisposing to ectopic gestation.
Sexually transmitted infections like Chlamydia,
gonorrhea also cause tubal damage.
Tubal disease also may occur as a result of endo
metriosis, appendicitis, previous pelvic surgery.
2. Previous ectopic pregnancy Women who have had one ectopic pregnancy have an increased risk of having another.
3. Tubal surgery: women who conceive after tubal ligation for sterilization, reversal of tubal ligation or any other type of tubal reconstructive surgery also have a higher risk of having an ectopic pregnancy.
4. Infertility The incidence of ectopic pregnancy is higher in women with infertility, mostly due to an increased incidence of tubal abnormalities. Women who conceive as a result of fertility drugs or in vitro fertilization( IVF) have a slightly higher risk of having an ectopic pregnancy as well as a combined intrauterine and ectopic pregnancy.
5. Intrauterine contraceptive device (IUCD) Women who use IUCD are less likely to have an ectopic pregnancy than most women, because the IUD is effective at preventing all types of pregnancy. However, if a pregnancy occurs in a woman using IUD, there is a high risk that it will be an ectopic pregnancy. In some women however, there is no apparent explanation for why an ectopic pregnancy has occurred.
2. Previous ectopic pregnancy Women who have had one ectopic pregnancy have an increased risk of having another.
3. Tubal surgery: women who conceive after tubal ligation for sterilization, reversal of tubal ligation or any other type of tubal reconstructive surgery also have a higher risk of having an ectopic pregnancy.
4. Infertility The incidence of ectopic pregnancy is higher in women with infertility, mostly due to an increased incidence of tubal abnormalities. Women who conceive as a result of fertility drugs or in vitro fertilization( IVF) have a slightly higher risk of having an ectopic pregnancy as well as a combined intrauterine and ectopic pregnancy.
5. Intrauterine contraceptive device (IUCD) Women who use IUCD are less likely to have an ectopic pregnancy than most women, because the IUD is effective at preventing all types of pregnancy. However, if a pregnancy occurs in a woman using IUD, there is a high risk that it will be an ectopic pregnancy. In some women however, there is no apparent explanation for why an ectopic pregnancy has occurred.
What are the symptoms of ectopic pregnancy?
The most common symptoms are:
●Missed menstrual period
● Abdominal pain
● Vaginal bleeding (scanty or normal)
●Symptoms of pregnancy( breast tenderness, nausea) Following rupture of the tube, the woman may experience severe pain, fainting and shock
●Missed menstrual period
● Abdominal pain
● Vaginal bleeding (scanty or normal)
●Symptoms of pregnancy( breast tenderness, nausea) Following rupture of the tube, the woman may experience severe pain, fainting and shock
How is ectopic pregnancy diagnosed?
If the urine pregnancy test is positive and an
ultrasound scan shows empty uterus, the
possibilities are:
● A very early normal intrauterine pregnancy, or
● A miscarriage, or
● An ectopic pregnancy Ultrasound (trans-vaginal ultrasound more sensitive than trans abdominal) can be used as early as 1 to 3 weeks after a missed period to determine whether a pregnancy is inside the uterine cavity. Ultrasound can also show fluid or blood in the abdominal cavity suggesting bleeding from an ectopic pregnancy Sometimes there may be no evidence of pregnancy on ultrasound. In such cases blood test is done to measure the pregnancy hormone levels (beta HCG). In a normal pregnancy, the blood level of HCG should double approximately every 48 hours. In ectopic pregnancy the levels are usually lower and rise more slowly.
● A very early normal intrauterine pregnancy, or
● A miscarriage, or
● An ectopic pregnancy Ultrasound (trans-vaginal ultrasound more sensitive than trans abdominal) can be used as early as 1 to 3 weeks after a missed period to determine whether a pregnancy is inside the uterine cavity. Ultrasound can also show fluid or blood in the abdominal cavity suggesting bleeding from an ectopic pregnancy Sometimes there may be no evidence of pregnancy on ultrasound. In such cases blood test is done to measure the pregnancy hormone levels (beta HCG). In a normal pregnancy, the blood level of HCG should double approximately every 48 hours. In ectopic pregnancy the levels are usually lower and rise more slowly.
Is it possible to remove the pregnancy from the abnormal location and put it into the uterus?
Unfortunately, this is not possible with the
present medical science
How is ectopic pregnancy treated?
Prior to sensitive tests and modern pelvic
ultrasound, ectopic pregnancies were usually
diagnosed only after they ruptured and had
caused internal bleeding. Surgery was then the
main treatment. Now, we can detect them earlier
with the help of urine / blood pregnancy tests
and ultrasound, thus allowing some ectopic
pregnancies to be treated safely without the
need for surgery.
Medical management With early diagnosis of an ectopic pregnancy, medical (non surgical) treatment is often possible with injection methotrexate. This injection is given intra muscularly and the dose may be repeated depending on the fall in the beta HCG levels. HCG levels are monitored after treatment until the level has fallen to undetectable. Methotrexate is most successful in women whose HCG and ultrasound results fall into specified limits and who are clinically stable with no evidence of internal bleeding. Surgical management Indications for surgery include:
●Ruptured ectopic pregnancy- surgery often needs to be done immediately if the woman’s blood pressure has fallen and she is unstable.
●Failed medical management with methotrexate.
●In rare cases of hetero-tropic pregnancy (one pregnancy in uterus and other, outside uterus)
Medical management With early diagnosis of an ectopic pregnancy, medical (non surgical) treatment is often possible with injection methotrexate. This injection is given intra muscularly and the dose may be repeated depending on the fall in the beta HCG levels. HCG levels are monitored after treatment until the level has fallen to undetectable. Methotrexate is most successful in women whose HCG and ultrasound results fall into specified limits and who are clinically stable with no evidence of internal bleeding. Surgical management Indications for surgery include:
●Ruptured ectopic pregnancy- surgery often needs to be done immediately if the woman’s blood pressure has fallen and she is unstable.
●Failed medical management with methotrexate.
●In rare cases of hetero-tropic pregnancy (one pregnancy in uterus and other, outside uterus)
How is surgery performed?
Surgery is performed either using a
laparoscopic approach (key hole surgery) or
through an open abdominal approach
(laparotomy).
Laparoscopy involves use of small telescope
with a camera and 2 to 4 small skin incisions.
Following laparoscopy women generally are
able to go home within 48 hours and return to
full activities in 4 to 7 days.
Despite the advantages of laparoscopy, not all
surgeries for ectopic pregnancy can be done
with this technique. Emergency situations with
severe internal bleeding or extensive scar tissue
(adhesions) may require immediate laparotomy.
Will my fallopian tube be removed?
If the ectopic pregnancy is diagnosed early
before the tube ruptures, a laparoscopic
salpingostomy may be performed. In this
procedure, the fallopian tube is opened and the
pregnancy tissue is removed while leaving the
tube in place.
However, in some cases, it is necessary to
remove the tube (Salpingectomy). This may be
required if there is uncontrolled bleeding,
recurrent ectopic pregnancy in the same tube, a
severely damaged tube, or a large tubal
pregnancy. If the remaining opposite tube is
normal, the chance of live birth is good.
Can an ectopic pregnancy affect my chances of future pregnancies?
Once you have had an ectopic pregnancy,
you are at higher risk of having another one. In
future pregnancies, be alert for signs and
symptoms of ectopic pregnancy until it is
confirmed that the pregnancy is growing intra
uterine.
The silver lining is that many women with
history of ectopic pregnancy will successfully
conceive and have children in the future, either
naturally or with the aid of an assisted
reproductive technology such as in vitro
fertilization (IVF).
Frequently Asked Questions About Endometriosis
What is Endometriosis ?
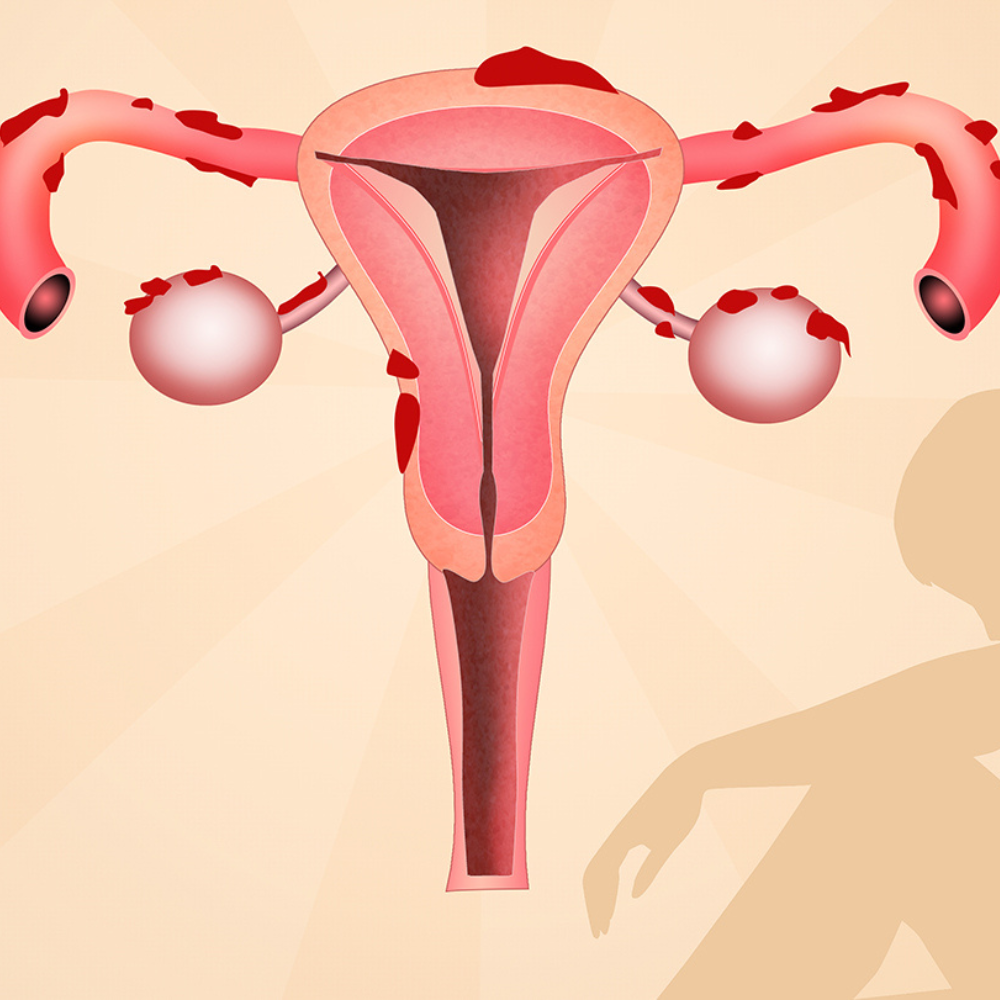
Endometriosis is a condition where tissue similar to the lining of the uterus (endometrium), is also found elsewhere in the body, mainly in the pelvis and abdominal cavity.
Every month a woman’s body goes through hormonal changes. Hormones cause the lining of the womb to increase in preparation for a fertilized egg. If pregnancy does not occur, this lining breaks down and bleeds. This is released from body as periods.
Endometriotic cells react in a similar way- except that they are located outside the womb. During the monthly cycle, hormones stimulate the endometriotic tissue, causing it to grow, then break down and bleed. Unlike the cells in the womb that leave as periods, this blood has no way to escape. This causes a chain of inflammatory reaction causing scar tissue and adhesions (abnormal bands of fibrous tissue) that cause the pelvic organs to stick to each other.
How common is Endometriosis?
10% of all women in their reproductive years are affected by endometriosis. These are typically the years between onset of menses until menopause.
Does endometriosis affect only the ovaries and fallopian tubes?
No.
Although ovaries and the fallopian tubes are most commonly affected, endometriotic lesions can be found in the following sites:
●On the pelvic side walls
●The surface of the uterus, especially posterior surface
●Ligaments of the uterus
●In the body of the uterus (adenomyosis)
●Urinary bladder
●Bowel (especially rectum)
●Ureter
●Laparoscopy / laparotomy scars
●Vagina
●Skin
Rarely in lungs, brain and spine
●On the pelvic side walls
●The surface of the uterus, especially posterior surface
●Ligaments of the uterus
●In the body of the uterus (adenomyosis)
●Urinary bladder
●Bowel (especially rectum)
●Ureter
●Laparoscopy / laparotomy scars
●Vagina
●Skin
Rarely in lungs, brain and spine
Is endometriosis hereditary?
It is known that first degree relatives of women with this disease are more prone to develop endometriosis. And when there is a hereditary link, the disease tends to be worse in the next generation.
Are there any risk factors for endometriosis?
The following factors may increase the risk:
●Early start of periods and late age of menopause
●Conditions which prevent the passage of menstrual flow out of body (imperforate hymen, vaginal septum, reproductive tract anomalies)
●Mother, aunt or sister with endometriosis
●Low body mass index
●Never giving birth or delayed childbearing
●Short menstrual cycle
●Long duration of menstrual flow Higher levels of estrogen in body or a greater lifetime exposure to estrogen
●Early start of periods and late age of menopause
●Conditions which prevent the passage of menstrual flow out of body (imperforate hymen, vaginal septum, reproductive tract anomalies)
●Mother, aunt or sister with endometriosis
●Low body mass index
●Never giving birth or delayed childbearing
●Short menstrual cycle
●Long duration of menstrual flow Higher levels of estrogen in body or a greater lifetime exposure to estrogen
What are the symptoms of endometriosis?
1.PAIN
The most common symptom of endometriosis is pelvic pain. The pain is usually cyclical and associated with periods, however some may have acyclical and atypical pain. Sometimes, the pain is so severe and debilitating that it affects a woman’s day to day activities
Pain may be felt:
●Before/during/after menses (dysmenorrhoea)
●During ovulation
●Pain during passing motions(dyschezia)
●When passing urine
●During or after sexual intercourse
●In the lower back and abdomen Endometriosis must be suspected in any patient with progressively increasing dysmenorrhoea and in any new onset cyclical pain.
2.Infertility Around 30 to 40% of endometriosis have difficulty conceiving. Women with moderate to severe endometriosis may require help of surgery, assisted reproductive techniques or both. Some of the possible causes of infertility are:
●Distorted anatomy of ovaries and tube
●Poor quality and quantity of eggs
●Chemicals produced by endometriotic tissues are toxic to sperm, egg and embryo
●Pelvic adhesions
●Altered immune function
3. Other symptoms may include
●Diarrhoea or constipation (especially during menses)
●Abdominal bloating
●Fatigue
●Heavy or irregular bleeding
●Before/during/after menses (dysmenorrhoea)
●During ovulation
●Pain during passing motions(dyschezia)
●When passing urine
●During or after sexual intercourse
●In the lower back and abdomen Endometriosis must be suspected in any patient with progressively increasing dysmenorrhoea and in any new onset cyclical pain.
2.Infertility Around 30 to 40% of endometriosis have difficulty conceiving. Women with moderate to severe endometriosis may require help of surgery, assisted reproductive techniques or both. Some of the possible causes of infertility are:
●Distorted anatomy of ovaries and tube
●Poor quality and quantity of eggs
●Chemicals produced by endometriotic tissues are toxic to sperm, egg and embryo
●Pelvic adhesions
●Altered immune function
3. Other symptoms may include
●Diarrhoea or constipation (especially during menses)
●Abdominal bloating
●Fatigue
●Heavy or irregular bleeding
Do all patients with painful periods (dysmenorrhoea) have endometriosis?
No.
Dysmennorhoea can be primary or secondary.
Primary is defined as painful periods in the absence of pelvic pathology. This can be considered as normal phenomenon and usually subsides with simple painkillers taken under doctor’s supervision.
Secondary dysmenorrhoea refers to painful periods due to pelvic pathology. Endometriosis is the most common cause of this. Other causes may include fibroid uterus, infections of genital tract, ovarian cyst etc.
Endometriosis is suspected when patient has progressively worsening pain with every period, severe pain right from the start of first menses, heavy and irregular menstrual bleeding, associated symptoms of diarrhoea, constipation or vomiting.
What is a chocolate cyst?
A chocolate cyst (ovarian endometrioma) is seen in endometriosis, wherein there is collection of altered blood in the ovary. They get their name from their brown and tar like consistency that is similar to melted chocolate. This cyst is benign (noncancerous). A chocolate cyst can affect one or both ovaries and can be single or multiple. It affects ovarian function and can cause pain.
Can endometriosis be prevented?
Currently there is no way of preventing endometriosis.
How is endometriosis diagnosed?
The gold standard method to diagnose endometriosis is laparoscopy, which enables a direct visualisation of the disease. However, this is an expensive, invasive procedure requiring hospitalisation.
Ultrasound may show ovarian cyst (chocolate cyst) or adenomyosis
MRI is helpful to diagnose the extent and depth of the disease, especially involving rectum, urinary bladder and ureter.
A thorough clinical history and gynaecological examination can also help.
What are the treatment options in endometriosis?
The goal of treatment is aimed at relieving pain, controlling the progression of disease and preserving fertility for future childbearing. The treatment decided is dependent on several factors, viz; age, severity of symptoms and disease, desire to have children.
● Hormonal treatment
Although hormonal treatment is not a permanent fix, it may help to slow endometrial tissue growth and prevent new implants. The various medicines used are, progestins (tablets or injection), oral contraceptive pills, GnRH agonist injections, etc.
● Surgery
Surgery aims to remove or destroy the deposits of endometriosis and is usually done via laparoscopy.
● Pain medication
Non steroidal anti inflammatory drugs like ibuprofen, mefenamic acid, naproxen sodium etc can help to ease menstrual cramps. These may also be used along with hormonal treatment.
● Hormonal treatment
Although hormonal treatment is not a permanent fix, it may help to slow endometrial tissue growth and prevent new implants. The various medicines used are, progestins (tablets or injection), oral contraceptive pills, GnRH agonist injections, etc.
● Surgery
Surgery aims to remove or destroy the deposits of endometriosis and is usually done via laparoscopy.
● Pain medication
Non steroidal anti inflammatory drugs like ibuprofen, mefenamic acid, naproxen sodium etc can help to ease menstrual cramps. These may also be used along with hormonal treatment.
Do dietary and lifestyle measures help to control endometriosis?
Yes.
Exercise releases endorphins (feel good hormones) which help to relieve pain. Moreover, regular exercise lowers the amount of estrogen in the body.
A healthy balanced diet with plenty of fruits, vegetables and omega 3 fatty acid (found in mackerel, sardines, walnuts, flaxseeds, pumpkin seeds) is advocated. Certain immunity boosting Indian foods like turmeric, fenugreek seeds, ginger and amla also help.
Avoiding or limiting use of plastic in kitchen, home, or workplace would help to limit the exposure to bisphenols and dioxin (endocrine disrupting chemicals). Plasticisers and phthalates found in cosmetics can also lead to abnormal hormonal milieu.
Alternative therapies with acupressure and yoga are helpful in certain patients.
Frequently Asked Questions About PCOS
what is polycystic ovarian syndrome(PCOS)?
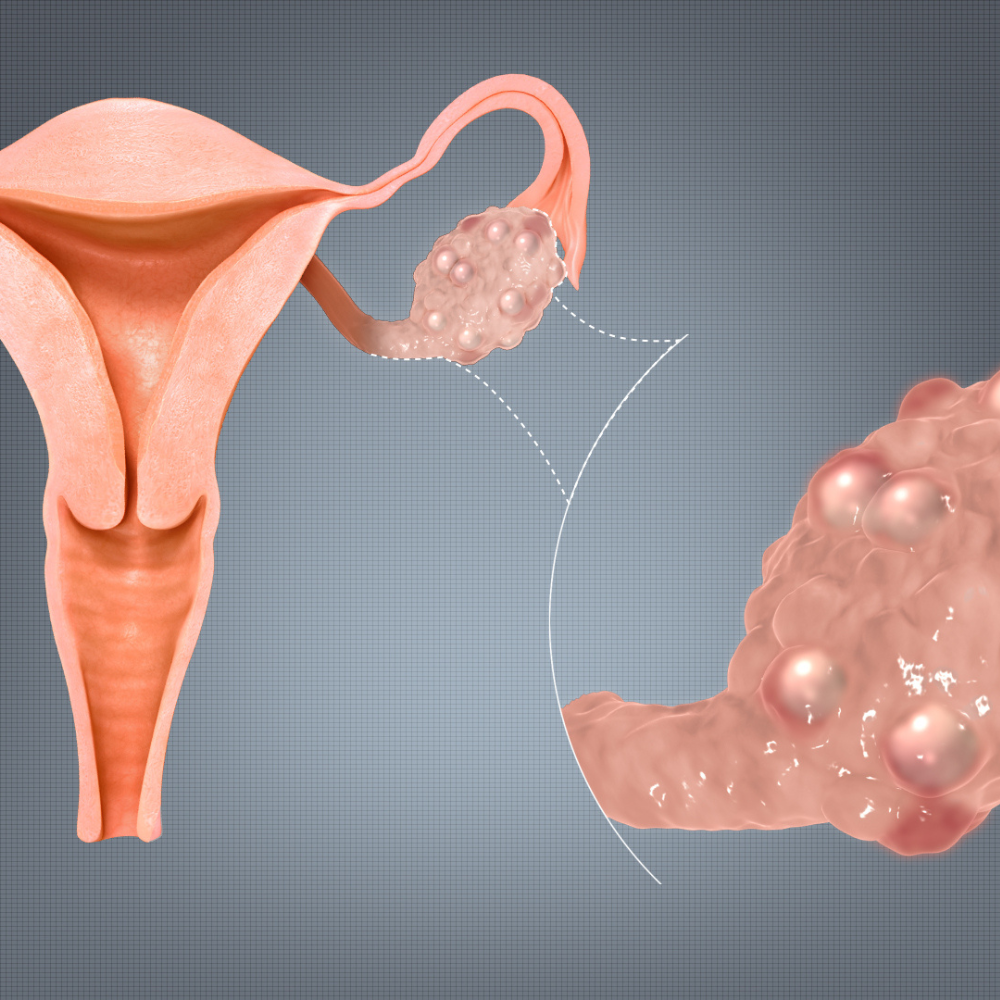
The ovaries are responsible for producing eggs (oocytes) and the female hormones (estrogen, progesterone and androgens) . In a normal ovary, ovulation (release of a mature egg) is a regular feature which takes place in a cyclical manner.
Polycystic ovarian syndrome is an endocrine disorder with heterogeneous features , wherein there is absence or infrequent ovulation associated with various hormonal imbalance . Polycystic ovaries are larger than normal ovaries with increased stroma and multiple small follicles filled with fluid, which fail to ovulate.
Why is PCOS so commonly heard of lately?
Approximately 10 to 20 % of women in the age group of 15 to 45 years, have PCOS.
Its incidence is on a rise due to change in lifestyle, food habits, increasing obesity and environmental factors.
what are symptoms of polycystic ovaries?
The symptoms include
Menstrual irregularities: No menstrual periods Frequently missed periods Very heavy periods or prolonged periods
Increase in body hair especially on face, chest, belly and upper thigh ( hirsutism )
Loss of hair on scalp
Being overweight, experiencing a rapid increase in weight or having difficulty losing weight
Oily skin, pimples (acne)
Difficulty becoming pregnant
Patches of thickened ,dark skin over neck , axilla, groin ( acanthosis nigricans)
Depression and psychological problems
Symptoms vary from woman to woman. Some women may have very few mild symptoms, while others are affected severely.
Menstrual irregularities: No menstrual periods Frequently missed periods Very heavy periods or prolonged periods
Increase in body hair especially on face, chest, belly and upper thigh ( hirsutism )
Loss of hair on scalp
Being overweight, experiencing a rapid increase in weight or having difficulty losing weight
Oily skin, pimples (acne)
Difficulty becoming pregnant
Patches of thickened ,dark skin over neck , axilla, groin ( acanthosis nigricans)
Depression and psychological problems
Symptoms vary from woman to woman. Some women may have very few mild symptoms, while others are affected severely.
What causes polycystic ovaries?
The cause is multifactorial
Androgen excess seen in almost 60 to 80 % of women
Insulin resistance or elevated insulin levels
Family history in mother, sister, aunt
Epigenetics : environmental factors like obesity, unhealthy lifestyle, low birth weight etc, can interact with genes to lead to PCOS
Androgen excess seen in almost 60 to 80 % of women
Insulin resistance or elevated insulin levels
Family history in mother, sister, aunt
Epigenetics : environmental factors like obesity, unhealthy lifestyle, low birth weight etc, can interact with genes to lead to PCOS
How do I know if I have PCOS?
There is no single test to definitely diagnose PCOS.
A diagnosis is made when you have any two of the following:
1.Irregular, infrequent periods, or no periods at all
2.An increase in facial or body hair and or blood tests that show higher testosterone levels than normal.
3.An ultrasound scan that shows polycystic ovaries.
It is important to note that ONLY polycystic ovaries on ultrasound, in the absence of any of the above mentioned signs or symptoms, is NOT PCOS.
A diagnosis is made when you have any two of the following:
1.Irregular, infrequent periods, or no periods at all
2.An increase in facial or body hair and or blood tests that show higher testosterone levels than normal.
3.An ultrasound scan that shows polycystic ovaries.
It is important to note that ONLY polycystic ovaries on ultrasound, in the absence of any of the above mentioned signs or symptoms, is NOT PCOS.
If I have PCOS, will I have difficulty getting pregnant?
PCOS is one of the most common but treatable causes of infertility. The hormonal imbalance interferes with the growth and release of eggs from ovaries, thus making it difficult to conceive.
What are the treatment options to get pregnant if I have PCOS?
1.Weight loss
If a patient is overweight, losing weight through healthy eating and regular physical activity can help to regularize periods in majority of women. Even 10% weight loss helps to restore ovulation.
2.Medicines to induce ovulation like clomiphene citrate and letrozole Some women may need intra uterine insemination (IUI) or in vitro fertilization(IVF), if the infertility is of long duration ,or if there are other factors of infertility associated.
2.Medicines to induce ovulation like clomiphene citrate and letrozole Some women may need intra uterine insemination (IUI) or in vitro fertilization(IVF), if the infertility is of long duration ,or if there are other factors of infertility associated.
Can PCOS cause complications in pregnancy?
Yes.
Women with PCOS can have
Miscarriage (especially in first trimester)
Gestational diabetes
Preeclampsia( high blood pressure)
Macrosomia (large weight babies)
Increased incidence of cesarean section.
Babies can also have increased risk of developing hypoglycemia (low blood glucose) and hypocalcemia (low calcium), in the immediate post natal period and can have long term risk of developing obesity and metabolic syndrome.
Miscarriage (especially in first trimester)
Gestational diabetes
Preeclampsia( high blood pressure)
Macrosomia (large weight babies)
Increased incidence of cesarean section.
Babies can also have increased risk of developing hypoglycemia (low blood glucose) and hypocalcemia (low calcium), in the immediate post natal period and can have long term risk of developing obesity and metabolic syndrome.
Is there a cure for PCOS?
There is currently no cure for PCOS. Even after menopause, women with PCOS often have high levels of androgens as well as insulin resistance. Medical treatments aim to manage and reduce the symptoms or consequences of having PCOS. Medication alone has not been shown to be any better than healthy lifestyle changes.
What are the various treatment options available?
PCOS treatment is tailored to each woman according to symptoms, existing health problems and whether she wants to become pregnant.
1.Exercise
At least 150 min/week of moderate intensity exercises like brisk walking, playing light sports etc. OR
At least 75 min/week of vigorous intensity activities like running, field sports, swimming, jumping rope,etc. OR
Weight training helps to strengthen the muscle and increase bone density
2.Medications
Combination birth control pills
Progestins
Metformin
Myoinositols
3.Healthy food
Balance carbohydrates with protein and healthy fats
Choose nutritious or high fibre carbohydrates instead of sugary or refined carbohydrates
Eat small frequent meals instead of large meals Do not skip breakfast
At least 150 min/week of moderate intensity exercises like brisk walking, playing light sports etc. OR
At least 75 min/week of vigorous intensity activities like running, field sports, swimming, jumping rope,etc. OR
Weight training helps to strengthen the muscle and increase bone density
2.Medications
Combination birth control pills
Progestins
Metformin
Myoinositols
3.Healthy food
Balance carbohydrates with protein and healthy fats
Choose nutritious or high fibre carbohydrates instead of sugary or refined carbohydrates
Eat small frequent meals instead of large meals Do not skip breakfast
Why have I been prescribed Metformin although my blood sugar is normal?
Hyper insulinemia or insulin resistance is seen in almost 80% patients of PCOS. In hyper insulinemia , the cells can’t utilize insulin properly, thus the pancreas makes more insulin to compensate.
High levels of insulin trigger the production of androgens by the ovaries and causes the arrest of normal follicle development.
Metformin is an insulin sensitizer, which helps to increase uptake of insulin. Moreover it helps to lose weight in obese patients.
What could PCOS mean for my long term health?
Women with PCOS are at greater risk of developing long term health problems, as:
1. Diabetes In view of insulin resistance, majority of patients with PCOS develop diabetes , especially if obese and over age of 40 years.
2.Metabolic syndrome ( obesity+ hypertension+ diabetes+ high cholesterol)
3.Sleep apnea (snoring) and day time drowsiness
4.Depression and mood swings
5.Endometrial cancer Since women with PCOS do not ovulate, the lining of the womb (endometrium) may thicken, leading to increased risk of developing cancer of endometrium in few women.
1. Diabetes In view of insulin resistance, majority of patients with PCOS develop diabetes , especially if obese and over age of 40 years.
2.Metabolic syndrome ( obesity+ hypertension+ diabetes+ high cholesterol)
3.Sleep apnea (snoring) and day time drowsiness
4.Depression and mood swings
5.Endometrial cancer Since women with PCOS do not ovulate, the lining of the womb (endometrium) may thicken, leading to increased risk of developing cancer of endometrium in few women.
Frequently Asked Questions About Cervical Cancer
What is cervical cancer?
Cervical cancer is the cancer of the opening mouth of the uterus, called the cervix. The cervix connects the uterus to the vagina and is covered by a thin layer of tissue made up of cells. Healthy cells grow, divide and are replaced continuously. Cancer of the cervix occurs when cells become abnormal. Cancer cells divide more rapidly and grow into deeper and surrounding tissue.
How common is it?
India accounts for nearly one fourth of the world’s cervical cancer deaths. It is the second most common cancer in Indian women (breast cancer being the first). Unlike women in developed world who have regular screening programmes to detect cervical cancer early , women in India are often diagnosed too late because of the lack of self screening, and the stigma and shame associated with a pelvic examination. Therefore, many women are diagnosed only in advanced stages, thus making treatment and recovery difficult.
What are the symptoms of cervical cancer?
Cervical cancer in very early stages usually does not have any symptoms. The longer a woman has cervical cancer without diagnoses, the more likely she will have symptoms.
1.Abnormal vaginal bleeding Bleeding spotting between cycles; after intercourse; after menopause
2.Unusual vaginal discharge While vaginal discharge is considered normal, the type of discharge you experience could be an indicator of vaginal cervical health. With cervical cancer you may notice discharge that is foul smelling and pink, brown or bloody in color. Sometimes there can be foul smell associated.
Weight loss, painful bowel movement, painful intercourse and obstruction to urine flow may be seen in advanced stages.
1.Abnormal vaginal bleeding Bleeding spotting between cycles; after intercourse; after menopause
2.Unusual vaginal discharge While vaginal discharge is considered normal, the type of discharge you experience could be an indicator of vaginal cervical health. With cervical cancer you may notice discharge that is foul smelling and pink, brown or bloody in color. Sometimes there can be foul smell associated.
Weight loss, painful bowel movement, painful intercourse and obstruction to urine flow may be seen in advanced stages.
What are the risk factors for cervical cancer?
1) HPV infection.
The most important risk factor for cervical cancer is infection with Human Papilloma Virus (HPV) .More than 90% of cervical cancers are linked to the virus. There are many types of HPV. The high risk types can cause cancer of cervix, anus, vulva, vagina and penis. It is important to note that most healthy women infected with HPV do not develop cervical cancer, and most HPV infections will eventually go away on its own. When exposed to HPV, the body’s immune system typically prevents the virus from doing harm. However, in a small percentage of people, the virus survives for years, contributing to the process that causes some cervical cells to become cancer cells.
The following risk factors increase your risk of becoming infected with HPV
●Early age at first intercourse (especially younger than 18)
●Multiple sexual partners
●Smoking: women who smoke are about two times more likely to get cervical cancer , compared to non smokers
●History of sexually transmitted infections especially gonorrhea, Chlamydia and syphilis
●Poor hygiene and sanitation and low economic status
●Weakened immune system as in HIV infection or in patients on immunosuppressant medications and steroids
2) Not getting screened
Cervical cancer is most often found in women who have not been screened with the Pap test in more than five years or who have never been screened at all.
3) History of cervical dysplasia (abnormal cell growth) which has not been adequately followed up or treated.
The most important risk factor for cervical cancer is infection with Human Papilloma Virus (HPV) .More than 90% of cervical cancers are linked to the virus. There are many types of HPV. The high risk types can cause cancer of cervix, anus, vulva, vagina and penis. It is important to note that most healthy women infected with HPV do not develop cervical cancer, and most HPV infections will eventually go away on its own. When exposed to HPV, the body’s immune system typically prevents the virus from doing harm. However, in a small percentage of people, the virus survives for years, contributing to the process that causes some cervical cells to become cancer cells.
The following risk factors increase your risk of becoming infected with HPV
●Early age at first intercourse (especially younger than 18)
●Multiple sexual partners
●Smoking: women who smoke are about two times more likely to get cervical cancer , compared to non smokers
●History of sexually transmitted infections especially gonorrhea, Chlamydia and syphilis
●Poor hygiene and sanitation and low economic status
●Weakened immune system as in HIV infection or in patients on immunosuppressant medications and steroids
2) Not getting screened
Cervical cancer is most often found in women who have not been screened with the Pap test in more than five years or who have never been screened at all.
3) History of cervical dysplasia (abnormal cell growth) which has not been adequately followed up or treated.
How can cervical cancer be prevented?
There’s no single way to completely prevent cervical cancer, but there are certain measures that can reduce your risk.
●Screening tests
Cervical cancer is preventable by screening women for precancerous cervical lesions. Cervical cancer has a long pre cancerous period, generally 10 to 15 years. This provides a considerable window of opportunity to detect pre malignant lesions. Early detection of the pre malignant conditions allows the disease to be cured completely. If regular screening is made part of the routine check-up of all women who are susceptible, the onset of cancer can be detected and combated effectively.
●HPV vaccine
The link between the development of cervical cancer and some types of HPV is clear. Although the vaccine may protect against only four subtypes of the virus( 16, 18, 51, 55), these account for majority of cervical cancer cases. HPV vaccines work best if administered prior to exposure to HPV. Therefore, the World Health Organization recommends vaccination for girls aged between 9 and 14 years, when the sexual activity has not started An important point to be noted is that vaccine does not replace cervical cancer screening.
●Avoiding multiple sexual partners The more sexual partners a woman has, higher is the risk of transmitting HPV virus
●Delaying first sexual intercourse The younger the woman is when she has sexual intercourse for the first time, the higher the risk of HPV infection becomes. The longer she delays it, the lower her risk Stopping smoking
●Screening tests
Cervical cancer is preventable by screening women for precancerous cervical lesions. Cervical cancer has a long pre cancerous period, generally 10 to 15 years. This provides a considerable window of opportunity to detect pre malignant lesions. Early detection of the pre malignant conditions allows the disease to be cured completely. If regular screening is made part of the routine check-up of all women who are susceptible, the onset of cancer can be detected and combated effectively.
●HPV vaccine
The link between the development of cervical cancer and some types of HPV is clear. Although the vaccine may protect against only four subtypes of the virus( 16, 18, 51, 55), these account for majority of cervical cancer cases. HPV vaccines work best if administered prior to exposure to HPV. Therefore, the World Health Organization recommends vaccination for girls aged between 9 and 14 years, when the sexual activity has not started An important point to be noted is that vaccine does not replace cervical cancer screening.
●Avoiding multiple sexual partners The more sexual partners a woman has, higher is the risk of transmitting HPV virus
●Delaying first sexual intercourse The younger the woman is when she has sexual intercourse for the first time, the higher the risk of HPV infection becomes. The longer she delays it, the lower her risk Stopping smoking
How long does it take for pre cancerous lesions to become cancerous?
It takes many years for cervical cancer to develop and spread.
In the early stages cell changes that occur before cancer is detected are called dysplasia. Many women are diagnosed with precancerous cell changes in their 20s and 30s but the average age of diagnosis of cervical cancer is age 49, which indicates the slow progression of the disease.
what are the different screening tests available?
1) Pap smear is the most commonly used cervical cancer screening test.
2) HPV DNA test for high risk HPV types
3) Visual inspection with acetic acid (VIA) inspects the cervix using acetic acid to identify abnormal changes on the cervix
2) HPV DNA test for high risk HPV types
3) Visual inspection with acetic acid (VIA) inspects the cervix using acetic acid to identify abnormal changes on the cervix
What is a pap smear test?
Pap smear is a screening test to find conditions that may lead to pre cancer or cancer of cervix.
Regular Pap smear screening is the best way to identify abnormal changes in the cells of the cervix at an early pre cancerous stage.
Pap smear can be done during routine gynecology check up. It is procedure done without anesthesia and it involves collecting of cells from cervix and vagina by a gentle applicator or brush.
Pap smear screening recommendation (American cancer society 2020)
<25 years: no screening 25 to 30 yr: Pap smear every 3 years 30 to 65 years: Pap smear every 3 years or Pap + HPV testing every 5 years
>65 years: No screening if consistent negative screening in last 15 years. However women with no prior screening should undergo tests once at 65 years, and if negative, exit screening. Women who have had a total hysterectomy with removal of the cervix also do not need to ne screened al
Regular Pap smear screening is the best way to identify abnormal changes in the cells of the cervix at an early pre cancerous stage.
Pap smear can be done during routine gynecology check up. It is procedure done without anesthesia and it involves collecting of cells from cervix and vagina by a gentle applicator or brush.
Pap smear screening recommendation (American cancer society 2020)
<25 years: no screening 25 to 30 yr: Pap smear every 3 years 30 to 65 years: Pap smear every 3 years or Pap + HPV testing every 5 years
>65 years: No screening if consistent negative screening in last 15 years. However women with no prior screening should undergo tests once at 65 years, and if negative, exit screening. Women who have had a total hysterectomy with removal of the cervix also do not need to ne screened al
What is HPV test ?
This test looks for cervical infection by high risk types of HPV. The HPV test and the Pap test are done the same way and both can be done together (co test). However the HPV test is costlier as compared to a conventional pap test.
The take home message is that cervical cancer is one of the most preventable cancers today.
Knowledge and awareness about regular screening can help in early detection and significantly reduce the associated complications and disease burden.
Quick Enquiry
Sunshine IVF centre is a speciality fertility clinic established to provide state-of-the- art facility for assisted reproduction for couples having problems in having a baby.