
Q: What is Endometriosis ?
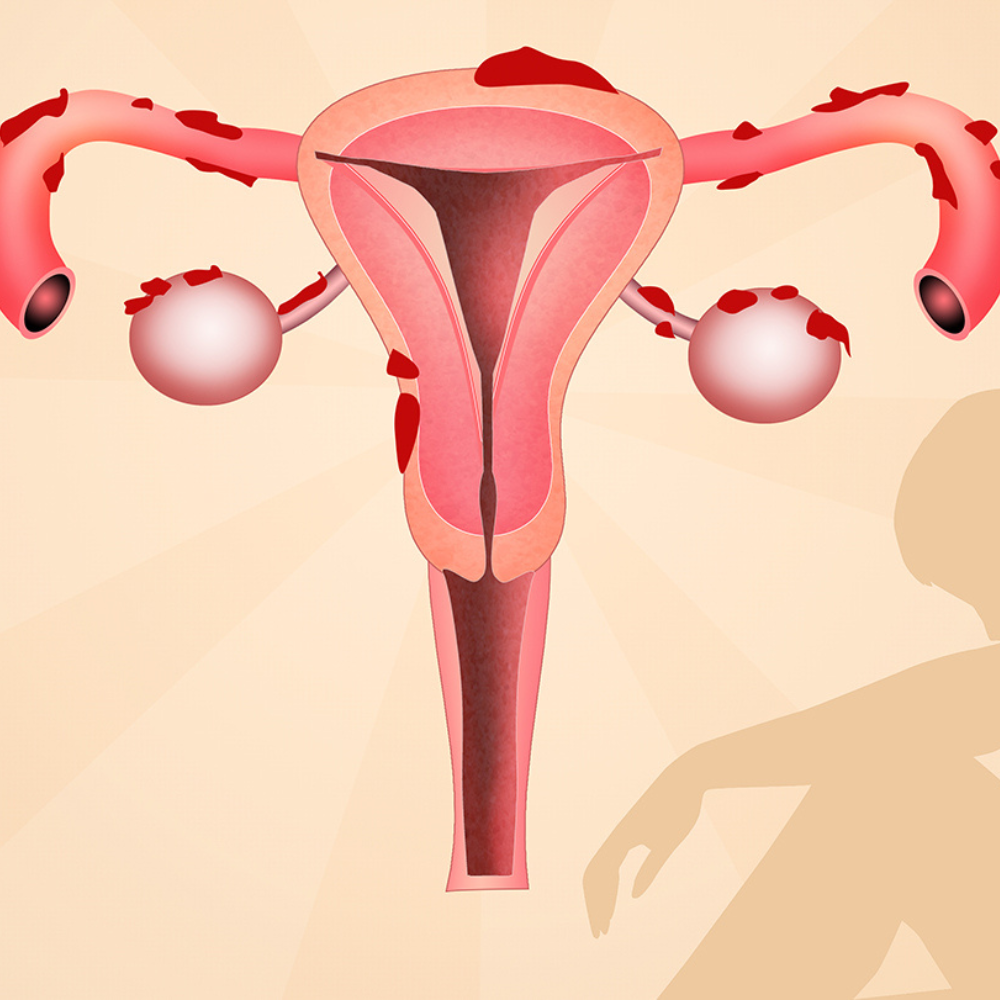
A: Endometriosis is a condition where tissue similar to the lining of the uterus (endometrium), is also found elsewhere in the body, mainly in the pelvis and abdominal cavity.
Every month a woman’s body goes through hormonal changes. Hormones cause the lining of the womb to increase in preparation for a fertilized egg. If pregnancy does not occur, this lining breaks down and bleeds. This is released from body as periods.
Endometriotic cells react in a similar way- except that they are located outside the womb. During the monthly cycle, hormones stimulate the endometriotic tissue, causing it to grow, then break down and bleed. Unlike the cells in the womb that leave as periods, this blood has no way to escape. This causes a chain of inflammatory reaction causing scar tissue and adhesions (abnormal bands of fibrous tissue) that cause the pelvic organs to stick to each other.
Q: How common is Endometriosis?
A: 10% of all women in their reproductive years are affected by endometriosis. These are typically the years between onset of menses until menopause.
Q: Does endometriosis affect only the ovaries and fallopian tubes? A: No.
Although ovaries and the fallopian tubes are most commonly affected, endometriotic lesions can be found in the following sites:
Q: Is endometriosis hereditary?
A: It is known that first degree relatives of women with this disease are more prone to develop endometriosis. And when there is a hereditary link, the disease tends to be worse in the next generation.
Q: Are there any risk factors for endometriosis? A: The following factors may increase the risk:
Q: What are the symptoms of endometriosis? A: 1.PAIN
The most common symptom of endometriosis is pelvic pain. The pain is usually cyclical and associated with periods, however some may have acyclical and atypical pain. Sometimes, the pain is so severe and debilitating that it affects a woman’s day to day activities
Pain may be felt:
Endometriosis must be suspected in any patient with progressively increasing dysmenorrhoea and in any new onset cyclical pain.
Around 30 to 40% of endometriosis have difficulty conceiving. Women with moderate to severe endometriosis may require help of surgery, assisted reproductive techniques or both. Some of the possible causes of infertility are:
Q: Do all patients with painful periods (dysmenorrhoea) have endometriosis?
A: No.
Dysmennorhoea can be primary or secondary.
Primary is defined as painful periods in the absence of pelvic pathology. This can be considered as normal phenomenon and usually subsides with simple painkillers taken under doctor’s supervision.
Secondary dysmenorrhoea refers to painful periods due to pelvic pathology. Endometriosis is the most common cause of this. Other causes may include fibroid uterus, infections of genital tract, ovarian cyst etc.
Endometriosis is suspected when patient has progressively worsening pain with every period, severe pain right from the start of first menses, heavy and irregular menstrual bleeding, associated symptoms of diarrhoea, constipation or vomiting.
Q: What is a chocolate cyst?
A: A chocolate cyst (ovarian endometrioma) is seen in endometriosis, wherein there is collection of altered blood in the ovary. They get their name from their brown and tar like consistency that is similar to melted chocolate. This cyst is benign (noncancerous). A chocolate cyst can affect one or both ovaries and can be single or multiple. It affects ovarian function and can cause pain.
Q: Can endometriosis be prevented?
A: Currently there is no way of preventing endometriosis.
Q : How is endometriosis diagnosed?
A: The gold standard method to diagnose endometriosis is laparoscopy, which enables a direct visualisation of the disease. However, this is an expensive, invasive procedure requiring hospitalisation.
Ultrasound may show ovarian cyst (chocolate cyst) or adenomyosis
MRI is helpful to diagnose the extent and depth of the disease, especially involving rectum, urinary bladder and ureter.
A thorough clinical history and gynaecological examination can also help. Q: What are the treatment options in endometriosis?
The goal of treatment is aimed at relieving pain, controlling the progression of disease and preserving fertility for future childbearing. The treatment decided is dependent on several factors, viz; age, severity of symptoms and disease, desire to have children.
Although hormonal treatment is not a permanent fix, it may help to slow endometrial tissue growth and prevent new implants. The various medicines used are, progestins (tablets or injection), oral contraceptive pills, GnRH agonist injections, etc.
Surgery aims to remove or destroy the deposits of endometriosis and is usually done via laparoscopy.
Non steroidal anti inflammatory drugs like ibuprofen, mefenamic acid, naproxen sodium etc can help to ease menstrual cramps. These may also be used along with hormonal treatment.
Q: Do dietary and lifestyle measures help to control endometriosis? A: Yes.
Exercise releases endorphins (feel good hormones) which help to relieve pain. Moreover, regular exercise lowers the amount of estrogen in the body.
A healthy balanced diet with plenty of fruits, vegetables and omega 3 fatty acid (found in mackerel, sardines, walnuts, flaxseeds, pumpkin seeds) is advocated. Certain immunity boosting Indian foods like turmeric, fenugreek seeds, ginger and amla also help.
Avoiding or limiting use of plastic in kitchen, home, or workplace would help to limit the exposure to bisphenols and dioxin (endocrine disrupting chemicals). Plasticisers and phthalates found in cosmetics can also lead to abnormal hormonal milieu.
Alternative therapies with acupressure and yoga are helpful in certain patients.


{kind=link}
{kind=link}